Summary
The coronavirus outbreak in the UK is modeled on the basis of rate of spread being proportional to the product of the number of uninfected people and the number of infectious people. The model is shown to accurately predict the deaths reported by PHE to-date, including the recent correction by PHE to include deaths outside of hospitals.
The model uses the 0.09% case mortality observed in Singapore for Coronavirus, which is comparable with the 0.1% mortality often cited for influenza. Accordingly the model finds that over 34 million people have already been infected in the UK and that around 55 million will have been infected at the end of the outbreak, forecast for November of this year. A total death toll of 49,300 is forecast for the UK, based on a gradual lifting of the lockdown from 11th May onwards.
The model finds that the British lockdown has saved at least 9,000 lives, even if it is assumed that the NHS would have coped without a lockdown i.e. unchanged mortality. The model also finds that the timing of the British lockdown was very important; if it had started 3 weeks earlier then it would have had virtually no effect on the outbreak. The 3 week extension of the lockdown is found not to have saved any lives.
Introduction.
This blog is an update on the blog I wrote a few weeks ago, entitled “Unlocking the Lockdown”. In the earlier blog I used a simple model of the infection to deduce the spread of the virus cases from the reported deaths. This approach relied on the assumption of a constant mortality and a known start date. It also imposed a continuous exponential phase, by assuming that the rate of spread at any moment in time was proportional to the number of cases at that same moment. This assumption yields an exponential curve, which is correct for the start of the epidemic but which becomes progressively less justified as more and more people become infected. Also, the earlier post did not consider the effect of the lockdown which began on the 23rd March.
I have therefore updated my calculations by using a more complete model for the spread of the virus, wherein:
- Rate of spread at any moment is proportional to the product of the number of uninfected people and the number of infectious people. The constant of proportionality, the “k” value, is the measure of the rate of spread of the virus. In the new model the k value was reduced by a factor of 2.75 for the period of the lockdown, to account for the reduction in contact between people imposed by the lockdown.
- The number of infectious people is those people who were infected within a characteristic time of the moment in time in question i.e. people infected earlier are not counted in the population of infectious people.
- The new model retains the concept of a constant mortality, and the number of deaths at a moment in time is the total number of infected cases a characteristic time before the moment, multiplied by the mortality.
- The new model retains the known start date used in the earlier model, namely 14th January 2020.
Method and parameters selected.
The new model lends itself to a numerical solution of the differential equations, as opposed to the analytical solution used for the earlier simpler model. For the new model the approach taken was to fit parameters to the data-set up to the 3rd April 2020 i.e. the same data-set used previously. I found:
Constant for rate of spread: k = (0.24567 / 67,000,000) per day per person
Mortality: x = 0.09%
Where the 67,000,000 is the total population.
The characteristic time for someone to be infectious was taken as 14 days from the moment of infection.
The characteristic time for someone to die from the virus was taken as 16 days from the moment of infection.
Note that the mortality used is very low compared with the 1 to 2% numbers frequently cited for coronavirus. However 0.09% is the case mortality found today in Singapore, based on 15 deaths and 16,169 reported cases in that country. Singapore has done extensive testing, over 24,000 tests per million people. This is double the UK number.
Note that the k value used above corresponds to 0.24567 per day at the start of the infection, when the number of uninfected people is more or less the whole population, and a first order model is appropriate. The k value used in the earlier model which was a first order model was 0.213 per day.
Results.
The new model was used to simulate the following scenarios:
- No lockdown.
- The current lockdown from 23rd March till 10th May with a gradual lifting from 11th May onwards, spread over 8 weeks.
- The current lockdown from 23rd March till 10th May with a sudden and complete lifting on 11th May.
- A shortened lockdown from 23rd March till 19th April with a gradual lifting from 20th April onwards, spread over 8 weeks.
- An earlier lockdown from 2nd March till 19th April with a gradual lifting from 20th April onwards, spread over 8 weeks.
No Lockdown.
The predicted curves of deaths, deaths per day and cases is shown in the following three graphs.



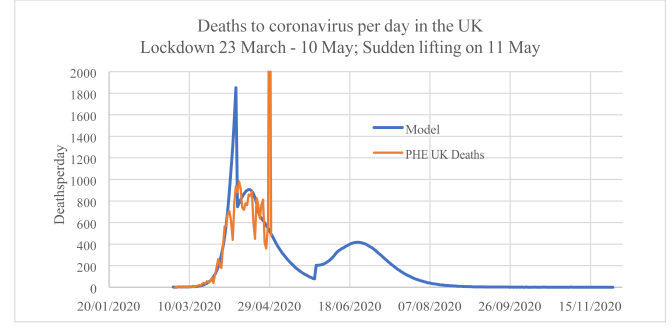
The model results (blue curves) show the characteristic “sombrero” for a constant value of k in the deaths per day graph. The red curves are the PHE data for deaths; the recent spike is due to the inclusion by PHE of deaths outside of hospitals in the data for 29th April onwards. The model shows that the infection would have spread over nearly the whole population by the end of April, yielding very high deaths per day. The total deaths would have been around 58,000 people if it is assumed that the 0.09% mortality would have applied. This in turn assumes that the NHS would not have been overwhelmed. It should be borne in mind that the mortality includes credit for medical care; if a medical care is reduced then mortality rises. I surmise that the assumption of an inflated mortality due the NHS being overwhelmed was behind the 250,000 deaths number predicted by Imperial College for the No Lockdown scenario.
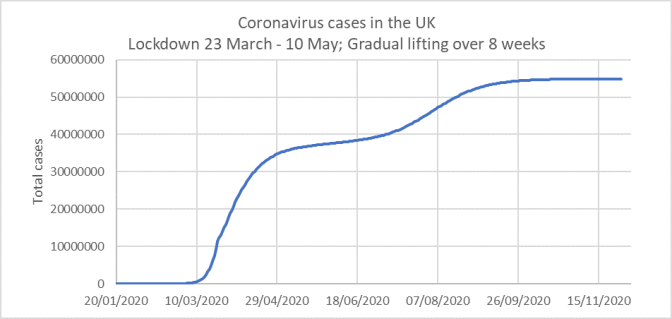
Current Lockdown 23rd March till 10th May with gradual lifting from 11th May onwards.
This scenario is what I think is going to happen. In the model, the 8 week gradual lifting is simulated by progressively increasing the k value from the low value used for the lockdown period (i.e. k = 0.08933 / 67,000,000 per day per person) to the non-lockdown value of k = 0.24567 / 67,000,000 per day per person.
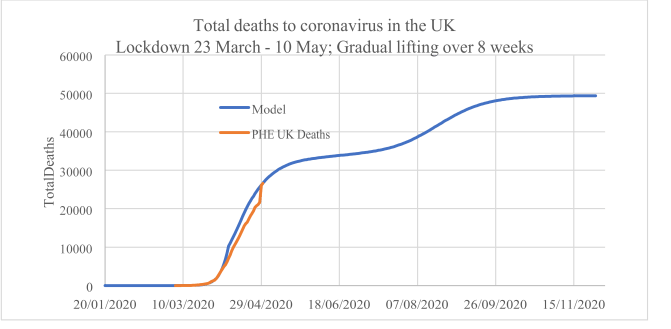

The graph of total deaths shows that the model has correctly predicted the course of the lockdown so far, as it matches the most recent PHE data i.e. 26,000 or so deaths. The prediction is that the total deaths will almost double from today i.e. finish at around 49,300. This is a considerable improvement over the 58,000 deaths predicted for the No Lockdown case, where the 58,000 number assumes no increase in mortality despite very high infection rates. The results of this model, if true, show that the lockdown has saved lives. Note that the death rate does bump up slightly and then subsides. The end of the infection occurs in late November 2020.
As with the no-lockdown scenario and indeed the earlier model, this model predicts very wide infection across the population. By the end of April over 34 million people are predicted to already be infected. This goes against mainstream thinking, but as yet no-one has come up with a reliable way of determining whether people have had the infection.
The model predicted a spike on the 8th April which is not reflected in the PHE data. However at this time the PHE numbers only included hospital deaths. The ONS have reported very high deaths in early April, and this is reflected in the retrospective upwards adjustment in PHE’s data this week, producing an artificial spike in the data.
Current Lockdown 23rd March till 10th May; Sudden lifting on 11th May.
This scenario is unlikely to happen. It was simulated by jacking up the k value from the lockdown value to the pre-lockdown value on 11th May.
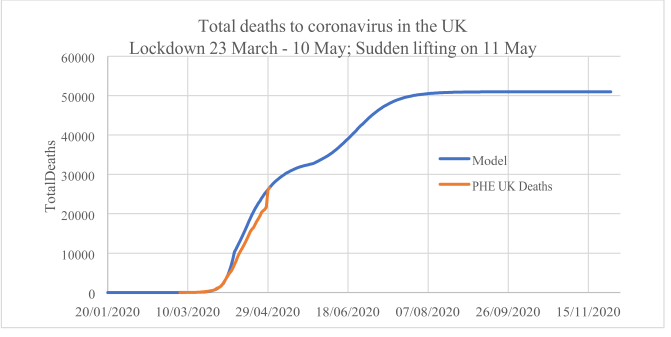
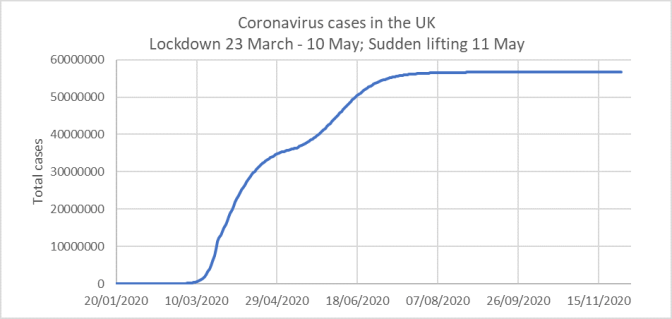
These results show that a gradual lifting of the lockdown will save some lives, as the total deaths is around 51,000 for the sudden lifting versus 49,300 for the gradual lifting. The difference is not huge, but we are still talking about 1,700 human beings’ lives. The infection ends more quickly than for the case where the lockdown is lifted gradually.
Shorter Lockdown 23rd March till 19th April followed by gradual lifting over 8 weeks.
This is the optimal scenario, in my opinion: the sombrero is flattened and the lockdown is progressively lifted.

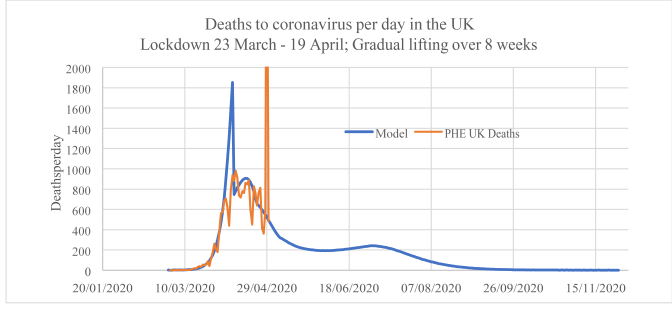
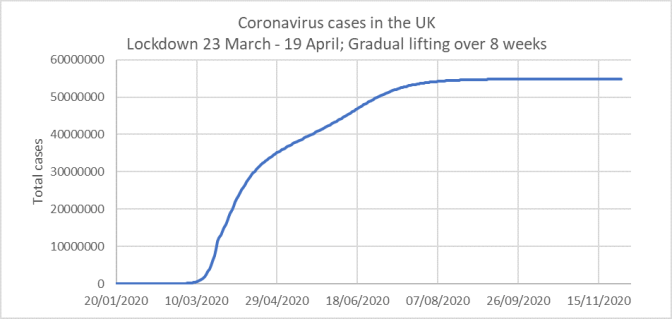
The model results show that the extra three weeks of the lockdown have brought no benefit: there is no reduction in the total number of deaths, as the number of deaths for the shorter lockdown is the same. The shorter lockdown is actually better in that the infection ends sooner as well.
Earlier Lockdown 2nd March till 19th April followed by gradual lifting over 8 weeks.
This scenario is in effect the current lockdown shifted 3 weeks earlier. Many people were urging this course of action on the government; the model’s results may surprise some people…



The results show that the lockdown squashes the infection, during the lockdown. During the 6 week lockdown no herd immunity is acquired at all, so when the lockdown is lifted, even gradually, the infection just re-establishes itself and the final outcome resembles the no-lockdown scenario, but delayed two months into June. These results show that the government was right: timing is important. Some countries that went in for earlier lockdowns may well be in for a nasty surprise later this year.
Conclusions.
- The new model shows that the 0.09% case mortality found in Singapore for coronavirus today applies to the United Kingdom as the overall mortality for the outbreak of coronavirus.
- Accordingly, based on a gradual lifting of the British lockdown made from 11th May onwards, a forecast of 49,300 total deaths is made for coronavirus in the United Kingdom. This does not include collateral deaths due to reduced treatments for cancer and other conditions during the 6-week lockdown. This forecast does not take credit for measures taken to protect the elderly and infirm, such as increased surveillance in care-homes.
- The model finds very widespread infection already present in the United Kingdom. Thus the number of infected people today, 30th April, is found to be over 34 million. At the end of the outbreak, forecast for November, over 55 million people will have been infected with coronavirus. Thus the herd immunity model for the infection is shown to be correct.
- The model finds that the lockdown has saved many lives. Without the lockdown lives lost would be at least 9,000 higher even if it assumed that mortality would have been unaffected by the very intense outbreak that would have resulted without the lockdown.
- Albeit that the lockdown was necessary for the first 3 weeks, its prolongation by a further 3 weeks is not found to have saved any lives.
- A gradual lifting of the lockdown will save lives compared with a sudden lifting. A sudden lifting sees total deaths increased by 1,700.
- The British government was correct in delaying the lockdown till the 23rd March. The model finds that the 6-week lockdown would have achieved nothing at all had it been imposed 3 weeks earlier, on 2nd March. The model finds that the effect of an earlier model would have been to delay the outbreak till June, but that the loss of life and intensity would have been the same as the no-lockdown scenario. So locking down too soon is a mistake.
James Bush
30th April 2020.
